
What is it?
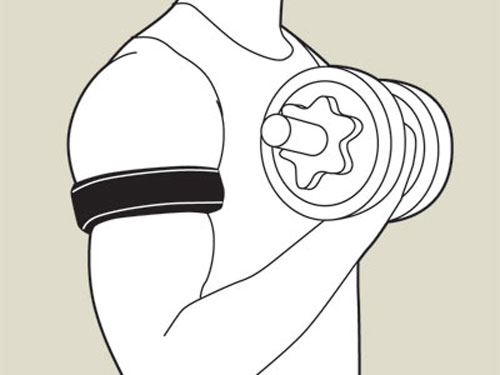
Blood flow restriction (BFR) is a training strategy involving the use of wraps or cuffs placed proximally around a limb; with the aim of maintaining arterial flow while occluding venous return during exercise (Scott et al. 2015). In layman’s terms this means that blood is flowing into the muscle; but none, or very little is getting out.
How is it performed?
A popular method is to use elasticated knee wraps and wrap them around the upper thighs or upper arms. A perceived wrap tightness of 7/10 will result in complete venous, but not arterial occlusion and has been used in a study by Lowery et al. (2014).
One must ensure the wraps are not too tight nor too lose. Loenneke et al. (2014) found that pressure appeared to increase muscle activation from 40-50% arterial occlusion but did not result in further increases at higher pressure. In other words, if they’re too tight
you will not elicit any benefits and you’ll increase risk of injury, if they are not tight enough blood easily leaves the muscle, eliminating the purpose of the wraps. Many strategies have been reported, however relatively light load resistant training using 20-30% 1RM is most common. Performing 4-6 sets to failure of exercises such as leg extensions, hamstring curls, squats, lunges, biceps curls, and triceps extensions.
Why use this technique?
Takarada et al (2002) did a study on a group of 17 male athletes and divided them into 3 groups – low intensity with occlusion (LIO); low intensity without occlusion (LI), and normal training.
The LIO group had both sides of their upper thighs trained with the proximal portions being compressed by a specially designed elastic belt. The subjects performed bilateral knee extensions for 4 sets at approximately 50% of their predetermined 1RM to failure, with 30 second rest intervals. Sessions lasted no longer than 10 minutes. The LI group then had to match the number of reps performed by the occlusion group. This was completed twice a week for 8 weeks, totalling 16 sessions.
This study aimed to measure several things including changes in muscle strength through measurement of isokinetic strength at preset angular velocities, and measurement of isometric torque at a knee angle of 80 degrees. They estimated changes in muscle endurance by having the subjects perform 50 repeated contractions of leg extensions and comparing the average value of peak torque during the last ten contractions compared to the initial ten contractions.
In addition, an MRI was used to retrieve cross-sectional images of the thigh in order to determine if an increase in strength was due to muscle hypertrophy or neuromotor adaptation. EMG signals were recorded from the vastus lateralis muscle as an indicator of muscle fibre recruitment during isometric torque exertion. Tests and image results were recorded prior to and after the 16 sessions.
The results of this study are undeniable as dramatic increases occurred within the LIO group in comparison to the LI and untrained control group. Percentage increases in strength after training were 14.3 (2.0)%, and 3.2 (2.3)% for the LIO and LI groups, respectively. Significant improvements in muscle endurance was seen in the LIO group only, which was believed to be caused by metabolic adaptations in the muscle fibres instead of an increased resistance to fatigue in the nervous system.
Both pre and post training MRI images were taken of the LIO group only. After the 8 weeks of vascular occlusion there was an approximate 15% increase of the cross-sectional area of the knee extensors. These results suggest that the increase in strength after occlusion training is due primarily to muscle hypertrophy.
Since hormones basically control everything, I want to quickly refer to a separate study previously conducted by Takarada et. al (2000). This study looked at growth hormone after low-intensity exercise with occlusion. The protocol was very similar to the one mentioned above, but used just 20% of the subjects 1RM.
The results of this study indicated that exercise with occlusion can provoke strong endocrine responses even at low intensities, as growth hormone increased 290 times as high as that before exercise. This is a significantly greater increase than that reported by Kraemer et al. (1990) for high-intensity resistant exercise with a short rest period (typical bodybuilding routine).
Conclusion
Blood flow restriction is a training strategy that can elicit major increases in muscle size and strength, as well as improvements in muscle endurance using just 20-50% 1RM. Major increases in growth hormone, peaking 15 minutes after the completion of low intensity resistance exercise with occlusion have been reported. This increase is even greater than that found after high-intensity resistance exercise without occlusion.
How I Use BFR
I recently employed this technique in my own training. Thus far I have completed 4 barbell back squat sessions using 35% of my 1RM, and 2 barbell front squat sessions using 30% 1RM. I performed 15-20 reps for 4-5 sets and keep my rest period under 1 minute. Since I do not have access to the special cuffs I have been using elasticated wraps and follow the suggested perceived wrap tightness of 7/10. Since the studies I have read kept the total occluded time within 10 minutes, I do as well; only removing the wraps after I have completed the exercise session.
It is difficult for me to measure if increases in muscular strength, size, and/or endurance is solely attributed to BFR as I train in weightlifting 3-4 times/ week and recently got back on my rollerblades since the weather has gotten more tolerable up in the North. However, I do plan on re-testing my 1RM back squat after a few more sessions, as prior to utilizing BFR my numbers were plateauing. Simply from the way my legs look and feel after these 6 sessions, coupled with the results of these studies, I am confident this will be the catalyst to any increases in my performance.
References
Scott, B. R., Loenneke, J. P., Slattery, K. M. & Dascombe, B. J. (2015). Blood flow restricted exercise for athletes: a review of the evidence. Journal of Science and Medicine in Sport.
Lowery, R. P., Joy, J. M., Loenneke, J. P., de Souza, E. O., Machado, M., Dudeck, J. E. & Wilson, J. M. (2014). Practical blood flow restriction training increases muscle hypertrophy during a periodized resistance training programme. Clinical Physiology and Functional Imaging, 34(4), 317-21.
Loenneke, J. P., Kim, D., Fahs, C. A., Thiebaud, R. S., Abe, T., Larson, R. D., Bemben, D. A. & Bemben, M. G. (2014a). Effects of exercise with and without different degrees of blood flow restriction on torque and muscle activation. Muscle and Nerve.
Takarada, Y., Sato, Y., Ishii, N., (2002). Effects of resistance exercise combined with vascular occlusion on muscle function in athletes. European Journal of Applied Physiology.
Takarada, Y., Nakamura, Y., Aruga, S., Onda, T., Miyazaki, S., Ishii, N. (2000). Rapid increase in plasma growth hormone after low-intensity resistance exercise with vascular occlusion. Journal of Applied Physiology.
Kraemer, W. J., L. Marchitelli, S. E. Gordon, E. Harman, J. E. Dziados, R. Mello, P. Frykman, D. McCurry, S. J. Fleck. (1990). Hormonal and growth factor response to heavy resistance exercise protocols. Journal of Applied Physiology.


Leave a comment